Healthy Relationships: A Plan for Improving Health and Sexual Education in New York City Schools
Executive Summary
For young people today, entering adulthood with a positive and comprehensive understanding of sexual health and wellness represents a vital base of knowledge and a critical element of any well-rounded education. When basic information about contraception, sexuality, gender identity, or intimate partner violence are left in the shadows – or worse, left to “locker room talk” – we disadvantage our youth and deprive them of a core base of information that helps to prepare them for adulthood. High quality, comprehensive sexual health education for students from kindergarten through twelfth grade serves as a basis for essential social and emotional competencies that influence lifelong patterns of behavior, social awareness, and decision-making, which strongly contribute to overall academic achievement.
The intent of the current presidential administration is clear: to scale back funding for programs that work to prevent teenage pregnancy through comprehensive sexual health education and instruction in favor of funding for abstinence-only programs. In July 2017, the Department of Health and Human Services announced that all grant funding through the Teen Pregnancy Prevention (TPP) program would be terminated two years early[i]. In addition, the House FY18 Appropriations proposal strips funding for evidence-based sexual health programs, including TPP and the Personal Responsibility Education Program (PREP) and increases funding for abstinence-only sexual risk education.[ii] In light of the federal government’s resolve to roll back progress on comprehensive sexual health education and waste money on programs that have been proven ineffective, it is imperative that New York City hold itself to a higher standard and ensure our students receive a comprehensive, medically-accurate, and age-appropriate sexual health education.
Unfortunately, New York City’s school-based instruction of sexual health education (or sex ed) is inconsistent and out of date compared to other major American cities. Worse, the New York City’s Department of Education’s (DOE) own data shows that for years the City has failed to comply with the State law requiring that students receive one semester of comprehensive health education by a certified health instructor at both the middle and high school levels. DOE is not fulfilling its own mandate that sex ed be taught in secondary schools grades six through twelve – a failure that is most acute in middle schools. The result is, our students are missing out on critical curriculum, from understanding gender identity, to discussing options for contraception and resources for LGBTQ youth. These shortcomings take on added urgency today, as more and more health indicators related to sexual health are beginning to inch up again after years of decline, especially in poorer neighborhoods of the city.
In May 2017, the New York City Council passed legislation creating a task force to review the state of sexual health education in city schools. This task force has been charged with reviewing current sexual health education curricula and, based on its findings, is expected to issue a report by December 2017. The task force will offer recommendations for improvements in sexual health curricula, implementation of sexual health education, accountability reporting, and the training and professional development of instructors.
This report, by New York City Comptroller Scott M. Stringer, is intended to provide a statistical foundation to the Council by assessing the state of health instruction in city schools today, examining some of the most worrisome health trends among teenagers, outlining the associated costs of addressing those trends, and establishing the connection between sexual health education and effective prevention. The report then recommends a series of reforms based on best practices from other cities aimed at helping students develop healthy, informed outlooks on their own sexuality and that of others.
Specifically, the New York City Comptroller’s report finds that:
- 88 percent of schools that teach middle and high school students do not have a teacher who is licensed for health education – with the majority of those schools being middle schools.
- Only 57 percent of eighth grade students completed the New York State-mandated requirement of one semester of health taught during the middle school years.
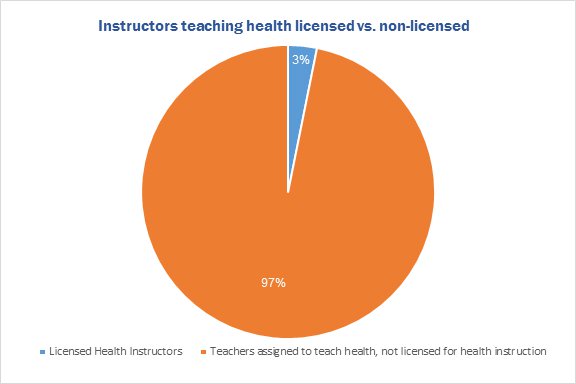
- In middle and high schools, 97 percent of health instructors are not licensed.
- Only 7.6 percent of all health instructors participated in any professional development related to sexual health education within the last two years.
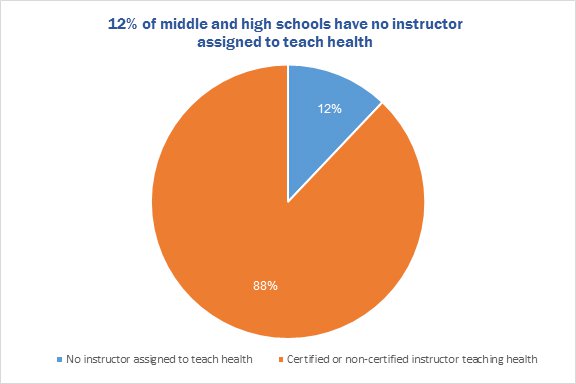
- 116 middle and high schools, or 12 percent, have no teacher at all assigned to teach health, including 100 middle schools (including K-8 and 6-8 schools).
- Of all 6-8 middle schools, 28 percent do not have a teacher assigned to teach health.
At the same time, public health data shows that:
- 4 percent of New York City teenagers reported experiencing sexual dating violence during the past 12 months, according to a 2015 survey of public high school students in grades 9-12. On average, New York City teenagers place over 1,400 calls to the City’s Domestic Violence hotline each month.[iii]
- While pregnancy rates among New York City teens have dropped in recent years, they remain high in some parts of the city. Teen pregnancy rates in the Bronx, for instance, are the highest in the state – in 2014, there were 69 pregnancies per 1,000 females age 15-19 years, compared with the citywide rate of 48.1 per 1,000.[iv]
- In New York City among youth ages 13-19, incidents of Chlamydia and Gonorrhea both were on the decline after reaching peaks in 2011. However, both began to inch up again in 2015, the most recent year for which there is city data, for the first time since 2010.
- LGBTQ youth are more likely to engage in risk behaviors that contribute to attempted suicide and substance abuse, and are at increased risk for homelessness[v].
This troubling landscape comes at a time when New York City students are themselves advocating for more and better guidance in navigating sexual health questions. A poll conducted by the Youth Advisory Council of the Sexual Education Alliance of New York City (SEANYC) in 2016 collected students’ suggestions for improving the quality of sex ed in their schools. The most frequent suggestion they received: by teaching it earlier and more often. According to the poll results, just 65 percent of middle and high school students reported that their health classes in school included sexuality education. Of those, 43 percent did not learn about gender identity/expression, and 38 percent did not discuss consent in class.[vi] Similarly, poll results revealed that just 66 percent of students knew where to go for sexual and reproductive health services.
The failure to adequately address the needs of students is compounded by a lack of accountability to both State and City requirements about how sex ed is supposed to be taught. While New York State regulations for Health Education and Wellness require that students receive one semester of health instruction in both middle and high schools, there is no explicit requirement that health instruction include sex ed. In addressing this gap, the DOE has advised principals since 2011 that middle and high schools must include sexual health as part of any comprehensive health instruction – although, critically, that guidance is not formally codified as a Chancellor’s regulation nor are there clear standards for accountability ensuring that sex ed is included as a standard part of students’ education.
To help prepare our students for the challenges ahead, and to provide a road map for updating and strengthening of sexual health instruction in New York City schools, the Comptroller offers the following recommendations:
Comply with State law by ensuring all secondary school health instructors are certified to teach health. The Department of Education should thoroughly assess certified health teaching positions across the district in order to comply with state law and develop strategies for improving professional development and certification opportunities. Schools that do not have certified health instructors in grades 6-12 should provide a pathway for certification for at least one health instructor. This may include covering or subsidizing the cost of certification.[vii]
Clarify and expand the current sexual health education requirement: Mandate sexual health and wellness instruction in the health curriculum taught in 6th to 12th grades through a Chancellor’s Regulation, and expand the mandate to include K-5th grades following National Sexuality Education Standards.
Improve methods of evaluation and public reporting: A review of sexual health education should be included as part of every school’s quality review, conducted by the Department of Education. The DOE does provide a snapshot of compliance with New York State requirements for health education in reporting the number and percent of students who completed health instruction, and the number and percent of teachers licensed to teach health. But this data would be more readily accessible to parents if it were included as part of every school’s quality review.
Expand School Wellness Councils to all schools. School Wellness Councils are existing volunteer bodies that can provide oversight and emphasize the importance of sexual health education but they are not in place in every school. Currently, School Wellness Councils exist in about 173 schools, which receive small grants (under $2,500) to implement or continue program.
Coordinate sexual health and wellness efforts with Department of Health and Mental Hygiene (DOHMH) and the Mayor’s Office to Combat Domestic Violence (OCDV). Both offices offer a wealth of information and resources. For example, OCDV provides trainings on healthy intimate partner relationships for teens through the NYC Healthy Relationships Training Academy, but trainings must be requested. DOH provides numerous resources to teens, including digital dating violence and cyberbullying awareness and prevention.
Educating our city’s youth is among the best possible defenses against rising rates of intimate partner violence, sexually transmitted infections, and unintended pregnancy among youth. Through comprehensive, culturally responsive, and sustained instruction, led by professional and trained educators, students can develop lifelong competencies promoting healthy behaviors, decision-making, and self-awareness.
Introduction: Where We Are Today
Decades ago, the general assumption was that “sex ed” should be limited to an overview of basic reproductive anatomy and possibly a quick review of contraceptive devices on the market. Today, young people in New York City are faced with a much more complex landscape. Like teenagers everywhere, many New York City adolescents are sexually active, with 46 percent of high school students and 62 percent of high school seniors reporting that they have had intercourse.[viii] Students have questions about gender identity and sexual orientation, and many are seeking guidance on how best to navigate a healthy, intimate relationship and where to turn for sexual and reproductive health services.
Today, students in New York City are themselves advocating for more resources and better guidance in navigating sexual health questions. A 2016 poll conducted by the Youth Advisory Council of the Sexual Education Alliance of New York City (SEANYC) collected New York City public school students’ suggestions for improving the quality of sex ed in their schools, and their most frequent suggestions included introducing sexual health education earlier and providing lessons each year.
The poll also gathered information about what students were learning about sexual health in school. According to survey results, just 65 percent of middle and high school students reported that their school health classes included sexuality education. Of those, 43 percent did not learn about gender identity/expression and 38 percent did not discuss consent in class.[ix] Similarly, poll results revealed that one third of students had no idea where to turn for sexual and reproductive health services.
Teaching comprehensive sexuality education in each grade can make the difference in equipping students to make important and informed decisions about their health and assess the risk behaviors they engage in. Students who are taught in the youngest grades to value mutual respect in all their relationships are given a platform from which to build healthy relationships and navigate conflict. For students in New York City, a single semester of health – sometimes taught as late as their senior year of high school – is inadequate preparation.
Without significant oversight and commitment from school administration and district leadership, it is too easy for sex ed to be neglected in schools. Failure to teach comprehensive sexuality education contributes to considerable economic and social cost. A review of the patterns of adolescent pregnancy, sexually transmitted infections, intimate partner violence, and victimization of LGBTQ youth in New York City provides a window into the root causes of some of the most persistent social problems facing our city and reinforces the need for the city to prioritize its commitment to providing cost-effective preventive education and increase accountability to New York City’s students.
Intimate Partner Violence
Among the most compelling arguments in favor of improving comprehensive sexual health education is preventing the patterns of intimate partner violence that develop from a very young age. Data compiled in the 2015 NYC Youth Risk Behavior Survey, a survey of public high school students in grades 9-12 and taken every two years, indicates that:
- 4 percent of young people reported experiencing sexual dating violence during the past 12 months;[x]
- 12 percent of students surveyed reported having been physically hurt on purpose by someone they were dating during the past 12 months;
Dating violence is often left unreported, and research indicates it is especially prevalent among young women who live in cities. A 2004 survey of 645 women ages 15-24 in New York City found that 67 percent experienced controlling behavior in their dating relationships and 37 percent reported sexual violence.[xi] African American women are estimated to experience lethal intimate partner violence at a rate that is three times greater than other racial groups in the U.S. For black women ages 15 to 35, domestic violence is the leading cause of death.[xii] An international analysis of adolescent intimate partner violence across nine countries concluded that helping youth understand what healthy stable relationships look like is crucial for violence prevention and is an important investment for the future of young women.[xiii]
Intimate relationships are now often influenced by internet usage and digital communications and young people need tools for understanding how to asses risk from online sources. Research from the Urban Institute indicates that a quarter of teens in dating relationships report being digitally victimized by their partners.[xiv] In many cases of cyberbulling, models of respectful communication have been undermined and victims feel unequipped to respond to the situation or know how to get help. For the abusers, meanwhile, consequences for cyberbullying are unclear. Both parties require intervention to identify patterns of abuse. Comprehensive sexuality education should include lessons on sexuality and technology to equip young people to know their rights in the digital landscape.
Unintended Teen Pregnancy
Historically, sexual health education has been effective in encouraging more widespread use of contraception to prevent unintended teenage pregnancies. As a result, teenage pregnancies and births have declined significantly over the past thirty years. The 2011 teen pregnancy rate in New York State was 50 percent below the 1988 peak.[xv] However, pregnancy rates among New York City teens remain high compared with other parts of the state. Teen pregnancy rates in the Bronx are the highest in the state – in 2014, there were 69 pregnancies per 1,000 females aged 15-19 years, compared with the citywide rate of 48.1 and the statewide rate (excluding New York City) of 24.[xvi] The 2015 teen birth rate, which includes only pregnancies that resulted in a birth, is at a 25-year low in New York State with about 14.6 births per 1,000 females ages 15-19.[xvii] In parts of Brooklyn and the Bronx, however, the birth rate is between 30 and 40 births per 1,000 teenage girls.[xviii]
Sexually Transmitted Infection
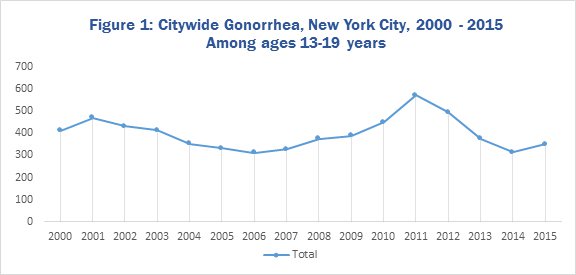
In New York City, certain sexually transmitted infections have begun to rise again among teens after a period of decline. Nationally, sexually transmitted infections remain a risk for sexually active youth, as in New York, and are on the rise. According to results from the 2015 CDC Sexually Transmitted Disease Surveillance report, cumulative cases of sexually transmitted infections saw year-over-year increases between 2015 and 2016 across the nation.[xix] Nationally, the highest rates of chlamydia and gonorrhea are among individuals between the ages of 15 and 24.[xx] In New York City, among youth aged 13-19, chlamydia and gonorrhea both reached a peak in 2011 and then began to decline. However, both began to inch up again in 2015, the most recent year for which there is city data.
As shown below in Figure 1, for youth aged 13-19 in New York City, the rate of gonorrhea infection has risen to 350 cases per 100,000, up from 315 cases per 100,000 in 2014. Because gonorrhea often goes undetected, regular screening and early treatment is critical. [xxi] Clear guidance on where to access testing and treatment should be included in any comprehensive sex ed curricula.
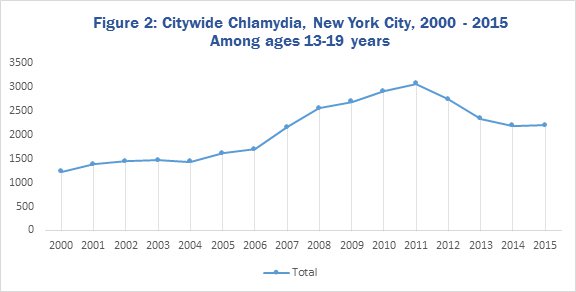
Likewise, though slower in pace, in 2015 there was a year-over-year increase in rates of chlamydia infection among youth ages 13-19 in New York City (see Figure 2). Rates remain significantly higher than fifteen years ago, with an infection rate of 2,195 cases per 100,000 in 2015. Kings County alone had the sixth highest number of reported cases of chlamydia nationwide.[xxii]
Source: New York City Department of Health, EpiQuery, Sexually Transmitted Diseases
Source: New York City Department of Health, EpiQuery, Sexually Transmitted Diseases
Syphilis, often linked with HIV, has also been increasing. Diagnoses among women increased by almost 30 percent from 2014 to 2015 and was particularly pronounced among women aged 20-29 and 15-19 nationally.
Given the uptick in sexually transmitted infections among New York City youth, it is perhaps unsurprising that 18 percent of New York City high school students report not using any contraceptive method during sexual intercourse, higher than the national average of 14 percent.[xxiii]
LGBTQ health risks
Lesbian, gay, bi-sexual, transgender, and questioning youth also show greater risk across several indicators. The 2015 Youth Risk Behavior Survey (YRBS) included a question on sexuality to better capture the experiences and needs of LGBTQ students in New York City and found that 15 percent of students identify as “gay or lesbian,” “bisexual,” or “not sure.”[xxiv]
Research shows that gay, lesbian and bi-sexual and transgender youth are at greater risk of bullying and victimization in school settings.[xxv] According to research from a 2015 National School Climate Survey, 85 percent of LGBTQ students nationwide reported experiencing verbal harassment, 13 percent reported being physically assaulted, and 60 percent reported being sexually harassed at school in the past year because of their sexual orientation. Fifty-six percent of survey respondents reported hearing homophobic remarks from school staff.[xxvi] In New York State, about 65 percent of LGBTQ students report experiencing verbal harassment and 9 percent experience sexual assault in school because of their sexual orientation.
LGBTQ youth who experience rejection, harassment, and discrimination are at greater risk for depression and suicidal tendencies, as reflected in health data of this demographic. A study by the Centers for Disease Control of health risk behaviors among students in grades 9-12 found that gay, lesbian, and bi-sexual youth have higher prevalence of risk behaviors, contributing to attempted suicide, alcohol and tobacco abuse, sexually transmitted infections, and weight management disorders.[xxvii] A recommendation of the study was that school health policies should specifically aim to reduce health risk behaviors of this demographic and seek to improve health outcomes for LGBTQ youth through sexual health education that is inclusive of LGBTQ experiences.
It should also be noted that transgender students in particular have unique behavior and health risks, especially in the current national climate of discrimination against transgender students in schools. Transgender youth attempt suicide at much higher rates than the general population, and research suggests that frequent harassment, discrimination, and marginalization is a direct cause.[xxviii]
In New York City, it is difficult to determine how many homeless youth identify as LGBTQ, but some estimate it to be close to 40%.[xxix] The Youth Risk Behavior Survey in 2015 indicates that a greater percentage of students who have been homeless or have been kicked out, ran away, or were abandoned identify as LGBTQ than heterosexual.[xxx]
Economic and social costs
The high costs of intimate partner violence, teen pregnancy, sexually transmitted infection, and victimization of LGBTQ youth among New York City high school students cannot be ignored.
- In 2010, it was estimated that teen childbearing in New York State cost taxpayers at least $337 million including increased costs associated with foster care, incarceration, and lost tax revenue. [xxxi]
- In addition, the Centers for Disease Control estimate the annual cost of treating new sexually transmitted infections in the U.S. is about $16 billion in direct medical expenses.[xxxii]
- A 2004 study estimated the cost of intimate partner violence in the United States, including medical care, mental health services, and lost productivity to be close to $5.8 billion.[xxxiii]
Such risks pose a social cost as well. Patterns of dating violence that develop in adolescence create a direct pipeline into lifelong patterns of abuse and violence. New York City teenagers place, on average, over 1,400 calls to the City’s Domestic Violence hotline each month.[xxxiv] According to the most recent Domestic Violence Task Force, in 2016, there were over 91,617 incident reports filed for intimate partner abuse across all age groups, up from 74,684 in 2015.[xxxv] In addition, 11.6 percent of all major crimes in New York City were domestic violence-related, which represents a 6.8 percent increase since 2007.[xxxvi] The New York City Police Department estimates that 70 percent of the increase in crime in public housing is attributed to domestic violence.[xxxvii]
Domestic violence has a direct impact on the homelessness crisis, as 25 percent of admissions to homeless shelters in New York City are linked to domestic abuse. Overall, women who experience intimate partner violence report losing an average of 7.2 work days each year.[xxxviii]
These risks and their associated costs are troubling. All of the above are clear indicators that we are perpetuating a public health crisis and ignoring the most basic intervention: early, comprehensive sexual health education. Knowing the potential impact on young people’s lives, educational leaders have an obvious responsibility to equip students with knowledge about the attributes of healthy relationships, how to prevent unintended pregnancy or disease transmission, and the resources they may need to identify and avoid abusive relationships or unhealthy patterns and behavior. Students who are equipped with comprehensive health education in school see positive benefits both for their health and academic success.[xxxix]
New York City Out of Compliance with State Law
New York State regulations for Health Education and Wellness require that students receive one semester of instruction in comprehensive health education in middle school, and one semester in high school. The state also has established specific learning standards for health, physical education, and family and consumer sciences.[xl] Neither the State’s health education regulation nor learning standards include specific requirements or guidance about sexual health instruction. The state regulation does, however, require that health classes for secondary education be taught by an instructor with certification in health, while elementary school health classes can be taught by a classroom teacher.
The state regulations also stipulate the following:
“A member of each faculty with approved preparation shall be designated as health coordinator, in order that the entire faculty may cooperate in realizing the potential health teaching values of the school programs. The health coordinator shall insure that related school courses are conducted in a manner supportive of health education, and provide for cooperation with community agencies and use of community resources necessary for achieving a complete school-community health education program.”
Since 2011, the New York City Department of Education has issued guidance that middle and high schools include sexual health as part of the comprehensive health instruction provided to students.[xli] Significantly, however, even if principals are aware of the policy that sex ed be provided in middle and high schools, there is a significant lack of oversight and little communication with superintendents to prioritize either health education or sex ed.
Due to public concern that the Department of Education was not fulfilling its policy to provide sexual health education, in 2016 the New York City Council enacted two local laws governing sexual education reporting requirements:[xlii]
- Local Law 14 requires the Department of Education to submit an annual report regarding school compliance with state regulations for comprehensive health and HIV/AIDs education for students in sixth through twelfth grades.
- Similarly, Local Law 15 requires a comprehensive report on teacher training and professional development in the area of sexual health for educators who teach health. This report must include information on how many full- and part-time instructors received training in the previous school year, and the percentages of instructors who attended multiple professional development trainings provided by the school.
A review of the data reported pursuant to Local Laws 14 and 15 reveals that the Department is highly inconsistent in providing health instruction to all middle and high school students. In addition, in many cases, the DOE is not complying with the minimum standards set by New York State that health classes in secondary schools be taught by a certified health instructor. Our review of the data shows:
- Only 57 percent of eighth grade students completed the New York State-mandated middle school health requirement of one semester of health taught during the middle school years.
- Just 7.6 percent of health educators received professional development within the past two preceding school years.
- In 961 schools that teach middle and/or high school grades, 844 schools — or 88 percent— have no teacher on staff who is licensed by the City to teach health.
- 116 middle and high schools, or 12 percent, have no teacher – whether licensed to teach health or not – assigned to teach health.
- Of 289 free-standing middle schools (6-8 grades), 28% have no teacher assigned to teach health.
- 97 percent of educators who teach health in middle and high school are not licensed to teach health; only 144 of the 4,560 teachers in schools that teach middle and high school students and were assigned to teach health are licensed to do so.
- 45 percent of health teachers do not hold state certification to teach health[xliii]
It is important to clarify the distinction between certification and licensing. Teachers may be certified by the State of New York in more than one subject. The city DOE assigns a license that matches certification in subject and grade level, but teachers can only be appointed under one license. The data reported by the city pursuant to Local Law 15, used in the analysis included in this report, provides an indication of teachers licensed to teach health. It should be noted that teacher certification data obtained from the New York State Education Department (SED) indicates that there are actually more certified health teachers than are represented by the count of teachers licensed to teach health, as reported by the city DOE. Even considering this distinction, New York City schools show a considerable gap in teachers with state certification in health. For consistency with the city’s reporting, this analysis includes only teachers with the more narrow measure of qualification – license, rather than certification – to teach health.
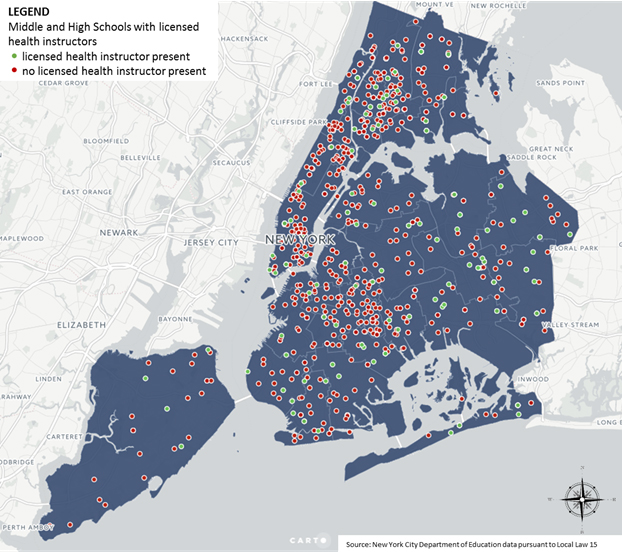
The map below provides a geographic view of all the schools that teach high school or middle school students (including K-12 schools) that currently have a licensed part- or full-time health instructor in green, and those that do not in red.
Majority of NYC Schools without Licensed Health Instructor
No Compliance Reporting with City Sex Ed Policy
While the new reporting of health education pursuant to Local Laws 14 and 15 is useful in providing a sense of how the City is in compliance with state mandates for health education, it is harder to track compliance with the City’s own policy requiring that sex education is included in the health curriculum. The data currently reported comes from course codes reported in the Department of Education’s database that collects schools’ self-reported scheduling information. A student who has been programmed for a course coded as a health class may or may not have received sex ed as part of the class’s curriculum. The lack of specificity means that it is difficult to conclude if sexual health instruction is being taught in particular schools.
Many New York City public school parents assume that sex ed is taught in their child’s required health courses, and may be surprised to learn that it is not. DOE’s current reporting does not indicate whether a particular school’s health class includes sex ed instruction. While the DOE recommends that schools use the nationally-recognized HealthSmart curriculum for middle and high school with the Reducing the Risk add-on for high schools, schools are not required to adopt this or any curriculum. Because schools are not monitored on whether sex ed is part of the health program, it is difficult to measure any individual school’s compliance with the city mandate and to ensure quality instruction is being provided in a comprehensive and consistent way. Parents, who are key partners in sexual health education and could be engaged through take home resources or online information, are essentially left in the dark.
It is also worth noting that in any school building owned by the Catholic Church, sex ed can only teach abstinence-only instruction. To teach the city’s recommended curriculum in these schools, students are required to leave the school property for sex ed lessons about contraception and disease transmission. The Catholic Church remains one of the largest landowners in New York City and leases approximately 40 buildings to the DOE.[xliv]
Middle schools are especially lagging
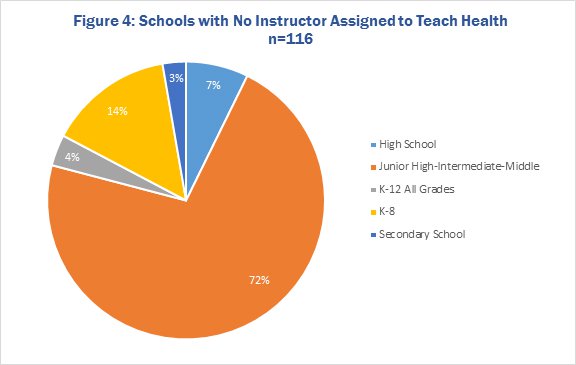
Middle schools make up a disproportionate number of the 116 schools with no assigned instructor for health (whether licensed to teach health or not). As shown in Figure 4, over 70 percent of schools with no assigned health instructor are middle schools. Furthermore, of the 289 schools the Department of Education classifies as 6-8 grade middle schools citywide, 28 percent have no teacher assigned to teach health, compared with just 3 percent of high schools that have no assigned health instructor.[xlv]
Across all middle schools, just 57 percent of 8th grade students have completed a health course – and whether sex ed is included in those courses is unknown. Not surprisingly, in schools with no teacher assigned to teach health, few students meet the health requirement. In middle schools with no teacher assigned to teach health, about 80 percent had five or fewer students who met the health requirement.[xlvi] It is unclear if the remaining middle schools contract with an outside CBO to fulfil the health requirement.
The DOE recommends that middle schools use the HealthSmart curriculum for age-appropriate and medically accurate pregnancy- and HIV-prevention instructional materials, though it is not clear how many middle schools are actively using the full curriculum. Despite using a curriculum that covers pregnancy- and HIV-prevention, middle schools may not provide condom demonstrations.[xlvii]
Neglecting middle school sexual health education is a costly mistake. Comprehensive sexuality education instills core social and emotional competencies in youth that influence lifelong patterns of behavior, social awareness, self-control, relationships, and decision-making.[xlviii] With so many middle schools left with no designated health instructor, too many students in this critical stage are missing an important window for learning.
Proper training is not reaching teachers
It is crucial that teachers who provide sexual health instruction are adequately prepared and supported with professional development opportunities. Opportunities for professional development are offered through the Office of School Wellness, which outlines a recommended sequence for teachers by grade level. The series of courses on comprehensive health education includes sexual health, LGBTQ inclusivity, HIV/AIDS, Respect in Relationships, and other topics. None of the courses are required for educators and just 7.6 percent of health instructors participated in any professional development related to sexual health education within the last two years, according to the DOE’s own data.[xlix]
The fact that so few teachers participate in professional development for sexual health education raises red flags about the significant lack of commitment and oversight from administrators in teaching this subject. It is critical that teachers who provide sexuality education are able to provide clear and up-to-date information that is age-appropriate and culturally responsive. Without a serious commitment from school leaders and district administration, teachers may be vastly underprepared and ill-equipped to provide accurate and un-biased answers to students’ questions.
In the absence of a school-based certified health instructor, some schools engage community based organizations to provide lessons in sex ed when a certified health instructor is not present. For many schools, CBOs play a critical role in teaching sexual health, particularly subjects that teachers do not feel equipped or comfortable teaching. Once again, however, the data reported pursuant to local law do not consider instruction provided by outside providers, making it difficult for parents or outside observers to know whether sex ed is being covered in a particular school’s health curriculum. In many cases contracting out for the sex ed portion of overall health instruction is highly effective. It should not, however, prevent the City from complying with State mandates that require all middle and high school students be taught by a certified health instructor.
In instances where schools engage CBOs to provide health related instruction in school, some additional concerns have come to light. In recent testimony to the New York City Council, an organization contracted by schools to provide DOE-approved sexual health education programming stated that instructors regularly encountered resistance from school administration about teaching all elements of the approved sex ed curriculum and are sometimes instructed to suppress content on sexual health.[l] In these instances where school administration is deviating from DOE’s guidelines, there are no measures in place to hold schools accountable. More robust accountability – from superintendents and senior administration – is needed to prioritize comprehensive sex ed and track compliance.
Models for Reform
Comprehensive sexuality education promotes essential social and emotional skills: self-awareness, self-management, social awareness, relationship skills, and responsible decision-making. Taught as a scaffolded curriculum from K-12, comprehensive sexuality education focuses on acquiring skills in the early elementary grades and developing greater competencies as students mature. In developing robust sexual health curricula, many cities have looked to the National Sexuality Education Standards (the “NSE Standards”) – a set of guidelines that districts can use as a benchmark in coordinating a consistent implementation model. Developed in 2007 by the Future of Sex Education – a partnership between Advocates for Youth, Answer, and the Sexuality Information and Education Council of the U.S. – these standards have been used in school districts in 32 states, including New York. The health curriculum recommended by the New York City Department of Education for use in middle school and high school is aligned to the NSE Standards, and the DOE would do well to align health teaching for all grades to them.
The NSE Standards provide a set of performance indicators that outline the minimum skills and content students should master at particular grade levels. They also provide instructors a scaffolded sequence for teaching about relationships and sexuality throughout a students’ school career. In the youngest grades, students are introduced to general concepts of anatomy, identity, healthy relationships, and personal safety. For example, by the end of second grade, students would show understanding of healthy relationships by being able to identify different kinds of family structures and describe the characteristics of a friend. More advanced topics related to sexual health, dating violence, and contraception are not introduced until later grades. This sequential approach to sexuality education can have greater impact on student health than a single course taught late in high school. Additionally, the social and emotional competencies that are acquired and reinforced through a well-developed K-12 comprehensive sexuality education have been linked to improved academic outcomes as well as reduced sexual risk taking and greater satisfaction in relationships.[li] [lii] [liii]
For instructors, continuity in programming from K-12 allows teachers to build off of content taught in previous years, without getting “stuck” teaching no more than the basic foundations of sex ed. The NSE standards are a key resource as school districts develop and administer comprehensive sexual health for all grades, and provide guidance and rationale for age-appropriate sexuality education content.
The DOE has acknowledged that there is room for improvement in its administration of sexual health instruction. In a recent hearing before the City Council, representatives from DOE outlined a few key strategies they believe will improve the current scope of sexual health education. These efforts include central meetings with principal focus groups to gather information from school leaders about the challenges of health education, helping superintendents and Field Support Center staff to emphasize the importance of health and sexual health education, and exploring options to increase teacher training opportunities.[liv]
As the DOE makes progress in these improvement strategies, it is useful to consider case studies from other cities that have recently overhauled sexual health education.
Chicago
Previously non-mandated, sex ed in Chicago Public Schools was implemented at individual schools solely at a principal’s discretion. Beginning in 2013, Chicago rolled out a system-wide mandate for K-12 sexual health curriculum aligned with the NSE Standards as part of a broader public health expansion and in coordination with the Chief Medical Officer. In aligning with the NSE Standards, the central district had greater authority to standardize sexuality education across all schools and ensure principals were implementing comprehensive sexuality education.
In Chicago’s case, professional development and teacher support is prioritized. Principals designate two teachers per school to attend a full day training on the sexual health curriculum. In addition, health curriculum materials are shared with teachers through an open Google interface, allowing external community organizations and sex educators to collaborate with teachers and provide supporting materials. Teachers may also request support from partner Community Based Organizations or other outside educators for specific content they do not feel prepared to cover.
To measure accountability of the roll-out, Chicago Public Schools includes a “sex ed” grade in each principal’s report card. Annual school inspections monitor the number of minutes spent on sexuality education at each grade level and whether CBO support was provided. Data on whether schools implement the sex education curriculum is included on each school’s public quality report.
Boston
In 2013, Boston Public Schools partnered with the Centers for Disease Control Division of Adolescent and School Health to secure grant funding for a new sexual health curriculum and teacher training. The multi-year implementation plan focused on sequenced instruction throughout the school year.
Like Chicago, the policy implemented by Boston Public Schools provides explicit guidance on teacher training. The district provides a three-day training, operated by Planned Parenthood, in addition to a two-day training on the District’s newly adopted sexual health curriculum. Each school is required to designate two teachers to attend the trainings. The commitment to teacher training emphasizes Boston’s commitment to building teachers’ capacity to deliver content on sexual health, rather than relying on outside providers.
Oversight of the new program is provided by the District Wellness Councils – community-based committees of 25 members, appointed by superintendents, that each represent local schools and communities. Individual School Wellness Councils review feedback from teachers, principals, and parents and recommend achievement benchmarks for evaluating program performance and any changes to the District Wellness Council, as necessary.
Broward County, Florida
Alarmed at CDC data that indicated Southern Florida has the highest rate of new HIV incidences, Broward County school district leaders and community members took the initiative to establish comprehensive sexuality education requirements in schools and create accountability measures to ensure all students receive instruction. The change expanded sexuality education to all grades and was phased in over three years, with new standards piloted in 21 focus schools during the first year and expanded district wide over the subsequent two years. The District matched curriculum to the National Sexuality Education Standards, adopting Chicago’s curriculum for younger grades.
Professional development training, offered by the district’s Diversity, Cultural Outreach & Prevention Department, is mandatory for all implementation staff, including teachers, counselors, nurses, classroom aides, and administrators. Initial trainings in-person are supplemented by bi-annual online recertification courses, which are all tracked to ensure compliance. Schools with less than 99 percent response for teacher trainings receive follow-up from the district.
Accountability is prioritized. Principals submit annual reports that identify the number of students who received sex ed in the school. Classroom teachers monitor program effectiveness by using pre- and post-tests at each grade level and classroom evaluations are completed by the district every three years.
Recommendations
While the Department of Education has recently undertaken welcome steps towards improving sexual education in New York City schools, today’s world requires a much more robust and system-wide approach if our children are to be prepared. When basic questions about contraception, sexuality, gender identity, or intimate partner violence are left in the shadows – or worse, left to “locker room talk” – we disadvantage our youth and deprive them of a core base of information that helps to prepare them for adulthood. For these and other reasons, the Comptroller recommends:
- The Department of Education should comply with state law by improving professional development and certification opportunities: The Department of Education should thoroughly assess certified health teaching positions across the district and draw up an aggressive plan to comply with state law. Schools that do not have certified health instructors on staff in grades 6-12 should be provided the resources necessary to hire at least one health instructor. This may include covering or subsidizing the cost of supplementary certification. While some schools may develop partnerships with outside sex ed providers, the DOE should make some consideration about what is preferred – developing in-house capacity or strengthening partnerships with outside providers.
To fill the gap in teacher certification and ongoing professional development, New York City should develop a training phase-in cycle to provide quality professional development for all teachers who teach health. In the first phase of the cycle, the city must prioritize certification for teachers in 116 schools that currently have no one teaching health. In phase two, the city should then ensure the certification of one or two instructors at each of the 844 schools that currently have no licensed health instructor. Phase three would offer ongoing professional development in sexual health instruction on an annual basis for all health and wellness teachers.
In addition, the Department must do more to boost recruitment efforts for its professional development offerings for instructors who provide health instruction for middle and high school students.
- Clarify and expand current sexual health education requirement: The City should mandate sexual health and wellness instruction in the health curriculum taught in 6th to 12th grades through a Chancellor’s Regulation, and expand the mandate to include K-5th grades following National Sexuality Education Standards. As early as second grade, children can learn healthy ways to communicate feelings, respect others, and manage their own behaviors. The value of a high quality, age-appropriate K-12 sexual health education requirement is clear. Students benefit from a scaffolded approach to the subject, with reinforced messages of healthy relationships and self-esteem. Teachers, also, benefit from a continuity between grades and schools. When students are familiar with the basics of sexual health knowledge, teachers can spend more time providing comprehensive sexual health instruction students need. The DOE should ensure that all K-12 sexual health instruction is aligned to the NSE Standards and that the standards of instruction for each grade level are clear in the District Wellness Policy.[lv]
In expanding and standardizing the quality of sexual health instruction being provided, New York should look to Chicago, Boston, and other major cities that have recently updated their sexual health curriculums for guidance. These cities have laid the groundwork for ensuring that there are ample opportunities for required teacher training.
Comprehensive sexuality education helps ensure that by the time young people contemplate becoming sexually active, they are equipped with knowledge and understanding about how to make healthy decisions and avoid risky behaviors and get trusted services.[lvi] Sexuality education therefore must not be limited to one semester taught in the junior or senior year of high school.
- Improve methods of evaluation and public reporting: Superintendents should ensure that sexual health education is part of every school’s quality review. The DOE does provide a snapshot of compliance with New York State requirements for health education in reporting the number and percent of students who completed health instruction, and the number and percent of teachers licensed to teach health. In order to report on compliance with New York City policy, each school’s quality snapshot, the public report of school-wide progress, should include an indication of whether comprehensive sexuality education, aligned with National Standards, is taught at the school, and whether the instructor is school staff or employed by an outside contractor.
Superintendents should also include one question in their school review to ensure that state certification and professional development opportunities are provided to teachers. This information could also be included in the school quality snapshot – a valuable and central resource for parents in reviewing their child’s school performance.
- Expand School Wellness Councils to all schools. New York City encourages, but does not require, schools to establish School Wellness Councils to set a wellness agenda for the school and ensure that physical and health education are provided at schools across the city. Currently, School Wellness Councils exist in about 173 schools. The Councils consist of student advisors, school staff and parents or community members who wish to contribute recommendations and feedback on school health agenda. The Department of Education provides grants ranging from $1,000 – $2,500 for schools to implement or strengthen existing councils.
Similar to Boston’s model, New York City should solicit feedback from School Wellness Councils on the sexual health program performance in the school, and recommendations for improvement. School Wellness Councils can ensure requirements for certified health instructors are being met and that schools’ sexual health curriculum is age-appropriate and medically accurate. The Councils can also provide important feedback to guide the city in future updates to its Wellness Policy.
- Coordinate sexual health and wellness efforts with Department of Health and Mental Hygiene (DOHMH) and the Mayor’s Office to Combat Domestic Violence (OCDV) and the Department of Education (DOE). Both DOHMH and OCDV offices offer a wealth of information and resources. OCDV provides free trainings for teens through the NYC Healthy Relationships Training Academy, but trainings must be requested by individual schools. DOH provides numerous resources to teens, including digital dating violence and cyberbullying awareness and prevention. The Mayor’s Domestic Violence Task force reinforced the link between education and intimate partner violence prevention. In its 2017 recommendations, the Task Force stipulates that the DOE will partner with the Mayor’s Office to Combat Domestic Violence to incorporate domestic violence and teen dating violence into the comprehensive health education curriculum. Significant investment has been made to ThriveNYC, offering another opportunity to connect social and emotional resources and services to students.
Educating our city’s youth is the best possible defense against intimate partner violence, rising rates of sexually transmitted infections, and comparatively high rates of teen pregnancy. Through comprehensive sexuality education, led by professional and trained educators, students can develop lifelong healthy behaviors.
Acknowledgements
Comptroller Scott M. Stringer thanks Elizabeth Bird, Policy Analyst and the lead author of this report. He also recognizes the important contributions made by David Saltonstall, Assistant Comptroller for Policy; Jennifer Conovitz, Special Counsel to First Deputy Comptroller; Zachary Schechter-Steinberg, Deputy Policy Director; Tammy Gamerman, Director of Budget Research; Angela Chen, Senior Web Developer and Graphic Designer; and Adam Forman, Associate Policy Director.
Endnotes
[i] Reveal, July 14, 2017: Trump administration suddenly pulls plug on teen pregnancy programs. https://www.revealnews.org/article/trump-administration-suddenly-pulls-plug-on-teen-pregnancy-programs/
[ii] The National Campaign to Prevent Teen and Unplanned Pregnancy: Federal Funding Streams Dedicated to Preventing Teen and Unplanned Pregnancy at a Glance
[iii] New York City Mayor’s Office, Mayor’s Office to Combat Domestic Violence. (2007). 2007 Fact Sheet: New York, NY.
[iv] New York State Department of Health, Teen Pregnancy Rate per 1,000 females aged 15-19 years, https://www.health.ny.gov/statistics/chac/birth/b13.htm
[v] CDC Sexual Identity, Sex of Sexual Contacts, and Health-Risk Behaviors Among Students in Grades 9–12 — Youth Risk Behavior Surveillance, Selected Sites, United States, 2001—2009. Surveillance Summaries, 2011: https://www.cdc.gov/mmwr/preview/mmwrhtml/ss6007a1.htm?s_cid=ss6007a1_w
[vi] Sexuality Education Alliance of New York City, https://sexedallianceofnyc.tumblr.com/
[vii] According to New York State certification data, about 45 percent of New York City teachers in health education are not state certified in health. Of that number 10.5 percent have no valid teaching certificate for their current assignment and and 34 percent are teaching more than 20% but less than 100% in an assignment for which no teaching certificate is held.
[viii] Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance: United States, 2009. Surveillance Summaries, June 4, 2010. MMWR 2010;59(No. SS-5). Referenced from http://www.advocatesforyouth.org/publications/publications-a-z/413-adolescent-sexual-behavior-i-demographics
[ix] Sexuality Education Alliance of New York City, https://sexedallianceofnyc.tumblr.com/
[x] New York City Department of Health, EpiQuery, New York City Youth Risk Behavior Survey, https://a816-healthpsi.nyc.gov/epiquery/index.html
[xi] Davidson, L.L. (2004). Prevalence of intimate partner violence in urban young women: Experiences with disclosure in health care settings. Referenced from https://www.dayoneny.org/statistics/
[xii] “African American Women Disproportionately At Risk For Death by Domestic Violence,” HG Legal Resources, http://www.hg.org/article.asp?id=31238
[xiii] Stockl, Heidi et al (2014) Intimate partner violence among adolescents and young women: prevalence and associated factors in nine countries: a cross-sectional study. Referenced from https://www.dayoneny.org/statistics/ Accessed from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-14-751
[xiv] The Urban Institute, Digitizing Abuse, http://www.urban.org/digitizingabuse
[xv] The National Campaign to Prevent Teen and Unplanned Pregnancy, http://thenationalcampaign.org/data/state/new-york
[xvi] New York State Department of Health, Teen Pregnancy Rate per 1,000 females aged 15-19 years, https://www.health.ny.gov/statistics/chac/birth/b13.htm
[xvii] The National Campaign to Prevent Teen and Unplanned Pregnancy, http://thenationalcampaign.org/data/state/new-york
[xviii] Citizens’ Committee for Children, Keeping Track Online Database, http://data.cccnewyork.org/data/map/79/teen-birth-rate#79/a/3/123/21/207
[xix] Centers for Disease Control and Prevention, 2015 Sexually Transmitted Diseases Surveillance, https://www.cdc.gov/std/stats15/default.htm
[xx] Centers for Disease Control and Prevention, 2015 Sexually Transmitted Diseases Surveillance, Figures in the National Profile, Figures 5 and 17; https://www.cdc.gov/std/stats15/default.htm
[xxi] Centers for Disease Control and Prevention, Gonorrhea Fact Sheet. Accessed from: https://www.cdc.gov/std/gonorrhea/stdfact-gonorrhea-detailed.htm
[xxii] Centers for Disease Control and Prevention, Sexually Transmitted Disease Surveillance 2015. Accessed from: https://www.cdc.gov/std/stats15/std-surveillance-2015-print.pdf.
[xxiii] New York City Department of Health, EpiQuery, New York City Youth Risk Behavior Survey, https://a816-healthpsi.nyc.gov/epiquery/sasresults.jsp
[xxiv] New York City Department of Health, EpiQuery, New York City Youth Risk Behavior Survey, https://a816-healthpsi.nyc.gov/epiquery/sasresults.jsp
[xxv] Bontempo, D., & D’Augelli, A. R. (2002). Effects of at-school victimization and sexual orientation on lesbian, gay, or bisexual youths’ health risk behavior. Journal of Adolescent Health, 30, 364-374. Referenced from https://www.stopbullying.gov/at-risk/groups/lgbt/white_house_conference_materials.pdf
[xxvi] Kosciw, J. G., Greytak, E. A., Giga, N. M., Villenas, C. & Danischewski, D. J. (2016). The 2015 National School Climate Survey: The experiences of lesbian, gay, bisexual, transgender, and queer youth in our nation’s schools. New York: GLSEN. Referenced from: https://www.glsen.org/article/2015-national-school-climate-survey
[xxvii] CDC Sexual Identity, Sex of Sexual Contacts, and Health-Risk Behaviors Among Students in Grades 9–12 — Youth Risk Behavior Surveillance, Selected Sites, United States, 2001—2009. Surveillance Summaries, 2011: https://www.cdc.gov/mmwr/preview/mmwrhtml/ss6007a1.htm?s_cid=ss6007a1_w
[xxviii] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339405/ and http://www.tandfonline.com/doi/full/10.1080/00918369.2016.1157998
[xxix] The Ali Forney Center, An Epidemic of Homelessness, http://www.aliforneycenter.org/about-us/lgbtq-youth-crisis/
[xxx] New York City Department of Health, EpiQuery, New York City Youth Risk Behavior Survey, https://a816-healthpsi.nyc.gov/epiquery/sasresults.jsp
[xxxi] The National Campaign to Prevent Teen and Unplanned Pregnancy, The Public Costs of Teen Childbearing in New York in 2010, https://thenationalcampaign.org/sites/default/files/resource-primary-download/fact-sheet-new-york.pdf
[xxxii] Centers for Disease Control, “Estimates of Sexually Transmitted Infection in the United States,” https://www.cdc.gov/std/stats/sti-estimates-fact-sheet-feb-2013.pdf
[xxxiii] Max, W., Rice, D.P., Finkelstein, E., Bardwell, R.A., Leadbetter, S. (2004) The Economic Toll of Intimate Partner Violence Against Women in the United States.Violence and Victims, 19(3): 259-72.
[xxxiv] New York City Mayor’s Office, Mayor’s Office to Combat Domestic Violence. (2007). 2007 Fact Sheet: New York, NY.
[xxxv] New York City Mayor’s Office to Combat Domestic Violence, 2016 Fact Sheet, http://www1.nyc.gov/assets/ocdv/downloads/pdf/ocdv-fact-sheet-2016.pdf
[xxxvi] NYC Domestic Violence Task Force 2017 Goals and Recommendations, http://www1.nyc.gov/assets/ocdv/downloads/pdf/DVTF-2017-Recommendations.pdf
[xxxvii] The New York Times, Domestic Violence Drives Up New York Shelter Population as Housing Options Are Scarce, Nov 10, 2014 https://www.nytimes.com/2014/11/11/nyregion/domestic-violence-drives-up-new-york-shelter-population-as-housing-options-are-scarce.html
[xxxviii] NYC Domestic Violence Task Force 2017 Goals and Recommendations, http://www1.nyc.gov/assets/ocdv/downloads/pdf/DVTF-2017-Recommendations.pdf
[xxxix] Dilley PhD MES, Julia, “Research Review: School-based Health Interventions and Academic Achievement” September 2009. http://here.doh.wa.gov/materials/research-review-school-based-health-interventions-and-academic-achievement/12_HealthAcademic_E09L.pdf
[xl] New York State Learning Standards for Health, Physical Education, and Family and Consumer Sciences, http://www.p12.nysed.gov/ciai/health/healthPEFACSLearningStandards.pdf
[xli] New York City Department of Education, Health Education Requirements, http://schools.nyc.gov/Academics/Wellness/WhatWeTeach/HealthEducation/HealthEdRequirements
[xlii] New York City Council Hearing Testimony October 27, 2015. Accessed from http://legistar.council.nyc.gov/LegislationDetail.aspx?ID=2483814&GUID=C4AD0D87-B3AB-4052-B272-7030D987507A&Options=ID%7cText%7c&Search=
[xliii] New York State Teacher Certification Data, 2015-16
[xliv] New York Daily News, Sex Education banned in public high school buildings owned by Catholic Church, April 7, 2013
[xlv] Based on the classification found in the Local Law 14 report; this includes “K-8” and “Junior High-Intermediate-Middle.”
[xlvi] This is determined by combining data from Local Laws 14 and 15. The Local Law 14 report classifies 565 schools as “Middle Schools” When comparing those DBNs with the schools listed in the Local Law 15 report, it was found that 112 have no health teacher assignment.
[xlvii] New York City Department of Education, Memo to High School Superintendents, May 2015.
[xlviii] Future of Sex Education, Building A Foundation for Sexual Health is a K-12 Endeavor, http://www.futureofsexed.org/buildingfoundation.html
[xlix] New York City Department of Education, Local Law 15 Report – Health Education Instructor Data. Accessed from http://schools.nyc.gov/community/city/publicaffairs/Health+Data.htm
[l] New York City Council Hearing Testimony, April 19, 2017. Accessed from http://legistar.council.nyc.gov/LegislationDetail.aspx?ID=2537056&GUID=CBBACEFF-D552-446A-8182-D9CA579C7FE0&Options=ID|Text|&Search=
[li] Durlak, et al., “The Impact of Enhancing Students’ Social and Emotional Learning: A Meta-Analysis of School-Based Universal Interventions.” Child Development 82.1 (January/February 2011): 405–432. Referenced from Referenced from
http://www.futureofsexed.org/buildingfoundation.html
[lii] Lando-King, et al., “Relationships Between Social-Emotional Intelligence and Sexual Risk Behaviors in Adolescent Girls.” Journal of Sex Research 52.7 (January 2015): 835-840. Referenced from Referenced from http://www.futureofsexed.org/buildingfoundation.html
[liii] Gambrel, et al., “Interpersonal Neurobiology and Couple Relationship Quality: A Longitudinal Model. ”Contemporary Family Therapy (February 2016); Malouff, et al., “Trait Emotional Intelligence and Romantic Relationship Satisfaction: Meta-Analysis.” American Journal of Family Therapy 42.1 (January 2014): 53-56.
Referenced from http://www.futureofsexed.org/buildingfoundation.html
[liv] Testimony of Elizabeth Rose, Deputy Chancellor of Operations at New York City Department of Education, April 19, 2017. Accessed from http://legistar.council.nyc.gov/LegislationDetail.aspx?ID=2537056&GUID=CBBACEFF-D552-446A-8182-D9CA579C7FE0&Options=ID%7cText%7c&Search=1028
[lv] New York City Department of Education, Health Education Requirements, http://schools.nyc.gov/Academics/Wellness/WhatWeTeach/HealthEducation/HealthEdRequirements
[lvi] Comprehensive Sexuality Education, Research and Results http://www.futureofsexed.org/compsexed.html